Sixty-four patients (101 knees) who met the criteria were selected, and six patients were excluded based on exclusion criteria. The study group included 24 men and 40 women, with an average age of 66 years (range 50 - 87).
A total of 101 knees had received intra-articular injections:
- 37 patients with bilateral injections (74 knees) and 27 patients with unilateral injections. Among these, 56 knees had received autologous intra-articular PRP injections, while 45 knees had HA injections.
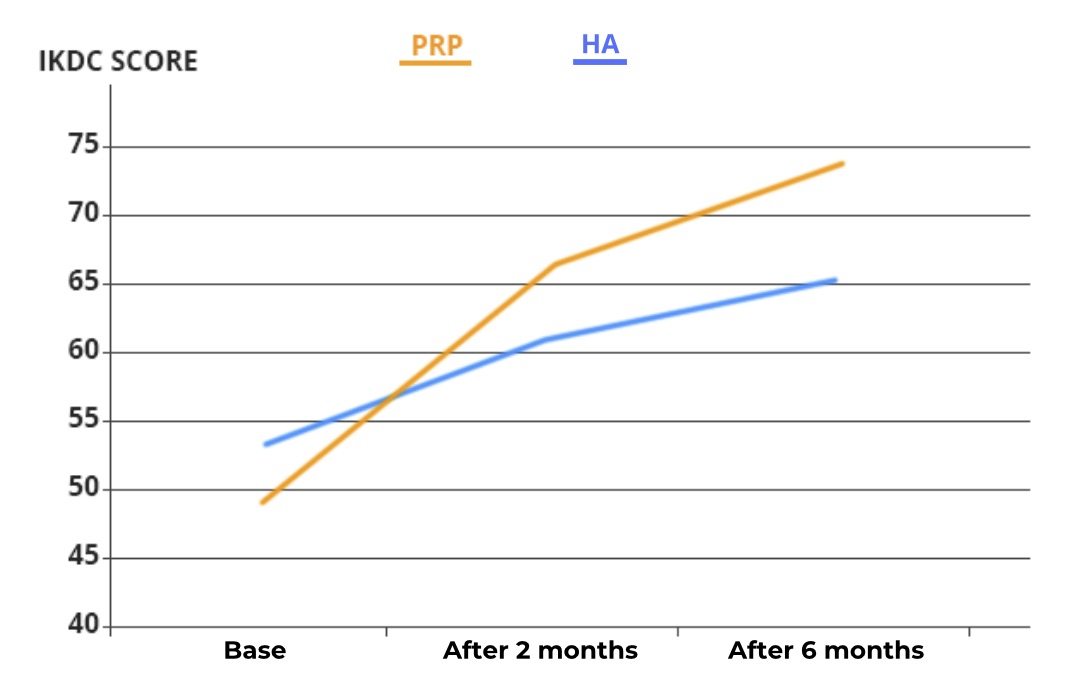
Knee assessment and pain scores were systematically recorded and documented at the Malacca center, using the International Knee Documentation Committee (IKDC) questionnaires and the Visual Analog Scale (VAS) before the injections, and after two months and six months following the injection. IKDC was preferred over other measurement tools like the Knee Injury and Osteoarthritis Outcome Score (KOOS) and the Western Ontario and McMaster Universities Arthritis Index (WOMAC) due to its high reliability and validity.
All patients included in the study received 4 ml of high molecular weight hyaluronic acid (average 1,476 x 106 Daltons) with a concentration of 22mg/ml. High molecular weight HA was specifically chosen because previous studies have shown greater and longer-lasting effectiveness in reducing pain and other symptoms and in joint function recovery compared to low molecular weight HA (LMW-HA).
PRP injections are prepared by taking 30 ml of the patient's venous blood, mixed with an anticoagulant, and centrifuged using the duo-spin method, at a speed of 2500 rpm for the first 5 minutes and then at 3200 rpm for the next 10 minutes (15 minutes in total).
Three distinct layers are produced at the end of centrifugation:
- plasma, the leukocyte layer (platelets), and red blood cells. Ninety-five percent of the plasma layer is discarded, and the remaining layers are mixed, resulting in approximately 2.5 to 3 ml of PRP at the end of the process, with an average platelet concentration of 1.4 to 1.6 million/μl.