





Platelet-rich plasma (PRP) is an autologous concentrate obtained by centrifugation of the patient's blood. It is a vehicle for platelet-derived growth factors used across numerous medical specialties to promote tissue regeneration and reduce local inflammation.
History of PRP
The first work on the use of autologous blood in tissue repair dates back to the 1960s in Germany, with Dr Schulte's research on wound defect treatment. In 1968, blood centrifugation was used to fill cysts.
The first documented clinical application dates from 1987, in the context of open-heart surgery in Italy. PRP therapy then developed in the 1990s, initially in oral and maxillofacial surgery, before extending to orthopaedics, dermatology and sports medicine.

Definition and Composition
PRP is a plasma fraction obtained from autologous blood with a platelet concentration 2 to 10 times higher than the baseline value. Platelets store more than 1,500 active proteins in their alpha and dense granules.
Key Growth Factors
- PDGF - cell proliferation and neovascularisation
- TGF-b - regulation of tissue regeneration and inflammation
- VEGF - angiogenesis and revascularisation
- EGF - epithelial proliferation
- IGF-1 - cell differentiation and collagen synthesis
Dense Granule Molecules
- Adenosine diphosphate (ADP) and triphosphate (ATP)
- Calcium
- Serotonin
- Dopamine
These molecules contribute to the regeneration of degenerative tissues and local haemostasis.
Preparation Protocol
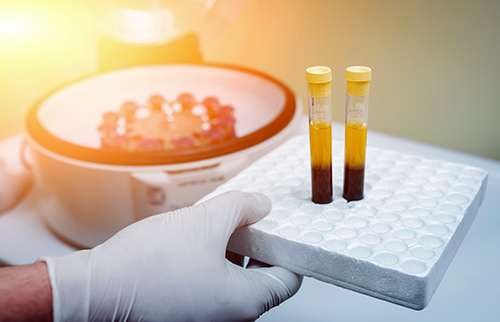
- Venous blood collection in anticoagulant tube (8 to 60 ml depending on kit and indication)
- Centrifugation according to protocol parameters (speed, duration, number of cycles)
- Separation of fractions: PPP (platelet-poor plasma), PRP (intermediate layer), erythrocyte pellet
- Activation with calcium chloride or autologous thrombin
- Sterile injection at the lesion site
Fields of Application
Musculoskeletal Medicine
- Orthopaedics: osteoarthritis, tendinopathies, ligament and meniscal lesions
- Sports medicine: tendon and muscle injuries
- Rheumatology: degenerative joint pathologies
Dermatology and Aesthetic Medicine
- Androgenetic alopecia
- Skin ageing, scarring, post-laser regeneration
Other Documented Specialties
- Plastic and reconstructive surgery
- Dental surgery and implantology
- Urology: interstitial cystitis, erectile dysfunction, incontinence
- Ophthalmology: retinitis pigmentosa, retinal ischaemia
- Gynaecology: ovarian insufficiency

Time to Observe Results
Clinical response to PRP varies according to the indication, patient profile and protocol used. As a general rule, a first clinical assessment is carried out at 4 to 6 weeks. Functional results are generally observed between 2 and 3 months, with a complete response potentially extending up to 6 months depending on the indication.
Tolerance and Adverse Effects
The autologous nature of PRP eliminates any risk of immunological rejection and transmission of infectious agents. Reported adverse effects are generally minor: transient pain at the injection site (24 to 48 h), expected early local inflammatory reaction. The main risks are related to injection conditions (asepsis, infiltration technique) and not to the product itself.
Share this content
These products might interest you




Discover more
-

PRP: Preparation Protocol, Indications and Clinical Applications
Published : 03/10/2022 -

PRP and Knee Pathologies: Indications and Injection Protocol
Published : 06/21/2021
